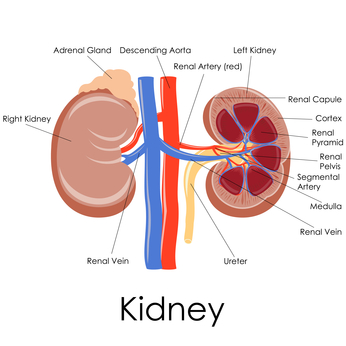
Kidney Scan
Ultrasound guided percutaneous kidney biopsy
Hepatitis B Vaccine and Kidney Disease
Acute Hemodialysis
Nutrition Guidelines for CAPD
Diet For Kidney Disease
High Phosphorus Foods To Limit Or Avoid
Kidney Diet
You will require adobe reader to view these pamphlets